
Reducing the Body Count During the Next Pandemic
Marshall, J.
Author correspondence: info@stem4humanrights.com
Cite this article: Marshall, J. (2024). Reducing the Body Count During the Next Pandemic. Diverse Perspectives on Wellness, 2(1), 1-10.
Abstract
The high death toll during the pandemic led to WHO’s 194 member states forming an Intergovernmental Negotiating Body to draw up a new pandemic agreement to facilitate a joint effort during global health emergencies. With nationalism, sovereignty-related concerns and an absence of collaboration as the most critical barriers to formalizing an effective agreement, the most ethical route for broadening global access to genomic and pathogenic data, vaccines, high priority research and pandemic-related products is to tie pandemic funding to global compliance standards by implementing an operational framework that requires contractual transparency, complementary exchanges of knowledge and technology and reassurances of sovereignty during the centrally administrated mitigation of a global health emergency.
Keywords: global health, pandemic agreement, vaccine nationalism, collaborative transparency
Introduction
In 2005, the World Health Organization’s international health regulations (IHR) agreement was made legally binding to improve the handling of public health emergencies in participating nations with the aim of affecting non-participating states but was heavily criticized during the pandemic given its ineffectiveness at enforcing compliance on early alerts, preparedness, coordination and implementation. As of May 5th, 2023 (the official end date of the COVID-19 pandemic), there were a staggering 770 million cases and 6.9 million deaths. The global perspective on coordination during the COVID-19 pandemic largely aligned with one of political failure driven by encountering an emerging infectious disease during late-stage capitalism, which in turn, led to monetization of the pandemic and country-level competition that eventually became a significant hurdle to coordination. As a result, vaccine nationalism incentivized pharmaceutical companies to exclusively produce vaccines within borders, governments were hesitant to share data or vaccines and relatively slow vaccine distribution to low and middle-income countries kept vaccination rates in the Global South at a significantly lower rate (Ofongo et al., 2024; Wenham & Eccleston-Turner, 2024).
Figure 1. Vaccination Coverage
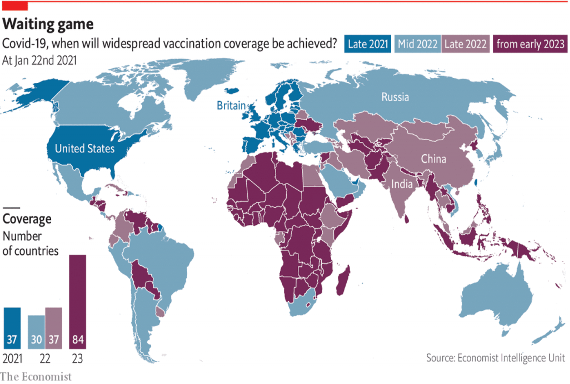
After the COVID-19 virus crossed border after border and disbelief, denial and nationalism transformed into an awareness that “no nation, regardless of its level of development, possesses the capacity to effectively combat global health threats in isolation”, in December 2021, the mid-pandemic realization of failure led the WHO’s 194 member states to form an Intergovernmental Negotiating Body and draw up a new pandemic agreement that would provide disease prevention and treatment for all individuals across the world regardless of national affiliation and prevent a repeat disaster (Ofongo et al., 2024).
Pandemic Agreement Negotiating Text
As shown in Figure 2 below, the United Nations Conference on Trade and Development (UNCTAD) delineates between the Global North (Northern America, Europe, Israel, Japan, South Korea, Australia and New Zealand) and the Global South (Africa, Latin America, Caribbean and the remaining countries in Asia).
Figure 2. The Global South and Global North
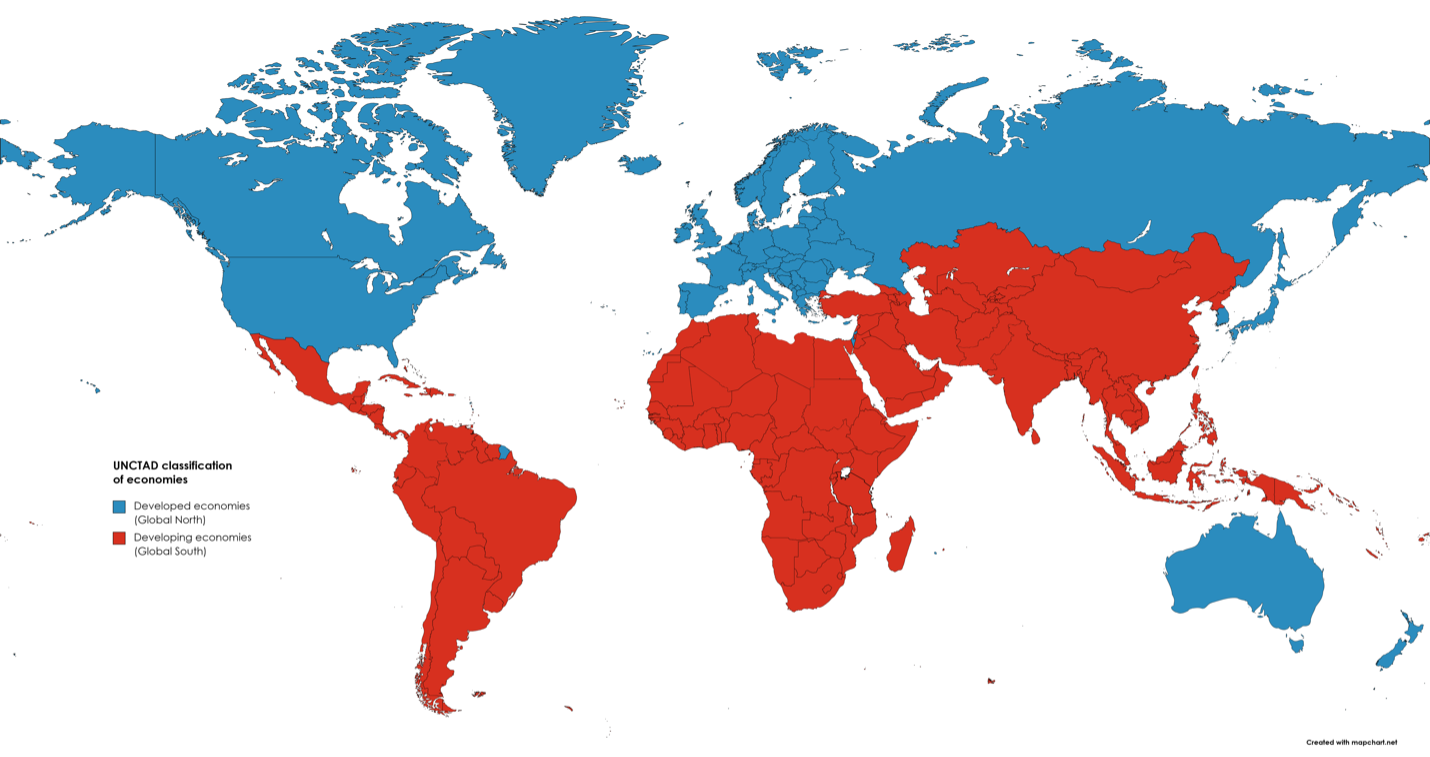
Despite wealth inequities, the Global North’s capacity for vaccine production and the Global South’s historical experience with handling emerging infectious diseases suggests a high complementary potential and an ability to put together an international collaboration agreement that rectifies “the gross inequities at national and international levels that hindered timely and equitable access to medical and other COVID-19 pandemic-related products” (Azzariti & Morich, 2023). However, one of the foremost barriers to achieving such a global agreement are perceived threats to sovereignty, which are often a primary source of conspiracy theories and may increase political opposition. That said, the competitive and opportunistic nature of global politics means the likelihood of a country diminishing its own authority during such a time of emergency and potential disorder is low to none. Thus, given that each country’s delegates and representatives are likely to insist on the greatest amount of border and information security at the expense of the member states’ collaborative potential, the final version of an effective global health emergency agreement is likely to include recommendations that insist on global coordination to the extent that they don’t interfere with national sovereignty. In this hypothetical instance, one might imagine countries agreeing to move in lockstep as it pertains to equitable access to financing and shared standards for disease surveillance and vaccine production, while acting independently according to their own traditions, cultural considerations and regional limitations as it pertains to others.
Although first-world funding for infectious disease surveillance in the Global South has been inconsistent over the last decade, countries in this region (e.g., Cameroon, Panama, etc.) have spent centuries battling malaria, yellow fever and other diseases that are notoriously difficult to contain due to their zoonotic nature. Thus, while the Global North outspent the Global South during the latest global health emergency, the Global South still miraculously accounted for a much lower proportion of the death toll while COVID-related excess deaths in the Global North skyrocketed beyond expectations (Schellekens & Sourrouille, 2024). In the context of health emergencies, currencies in the Global North are often more tangible (cash, vaccine production capacity) than those in the Global South (collectivism, emerging infectious disease expertise), and yet, given the Global South’s relative performance during the pandemic, the pandemic agreement’s effectiveness will perhaps be helped by the acknowledgement that, at least in the context of global health emergencies, the Global North is clearly in need of as much help from the Global South as it wishes to offer.
Operationalizing Equity
Given the acknowledgement that pandemic-era inequities suffered largely within the Global North and South were key proponents of the spread of COVID-19, and that the open-endedness of the previous agreement was a barrier to collaboration and compliance, the Zero Draft of the pandemic agreement explicitly discusses equity as one of its guiding principles and rights:
“Equity: The absence of unfair, avoidable or remediable differences, including in their capacities, among and within countries, including between groups of people, whether those groups are defined socially, economically, demographically, geographically or by other dimensions of inequality, is central to equity. Effective pandemic prevention, preparedness, response and recovery cannot be achieved without political will and commitments in addressing the structural challenges in inequitable access to fair, equitable and timely access to affordable, safe and efficacious pandemic-related products and services, essential health services, information and social support, as well as tackling the inequities in terms of technology, health workforce, infrastructure and financing, among other aspects.”
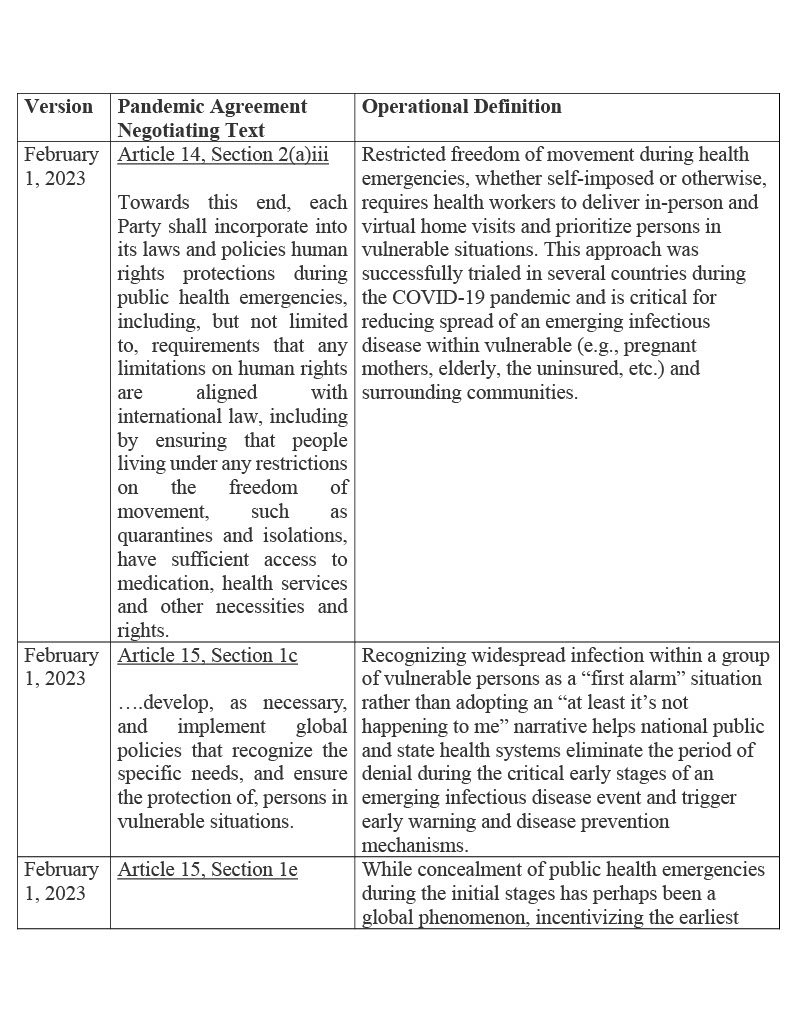
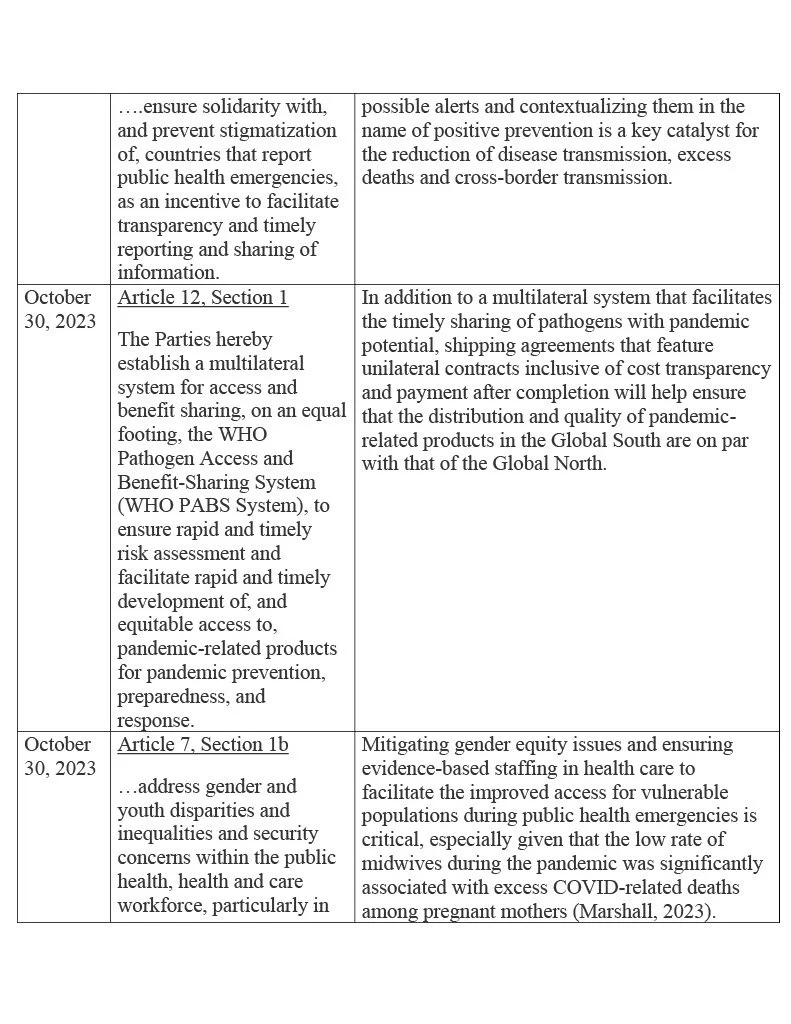
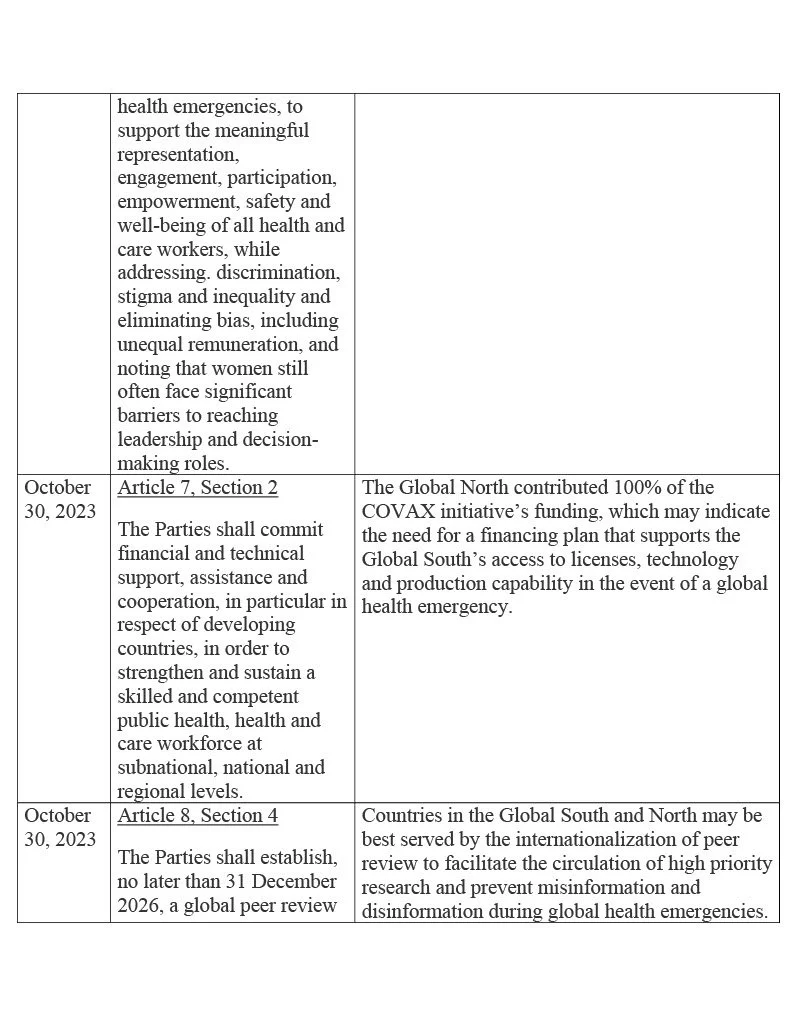
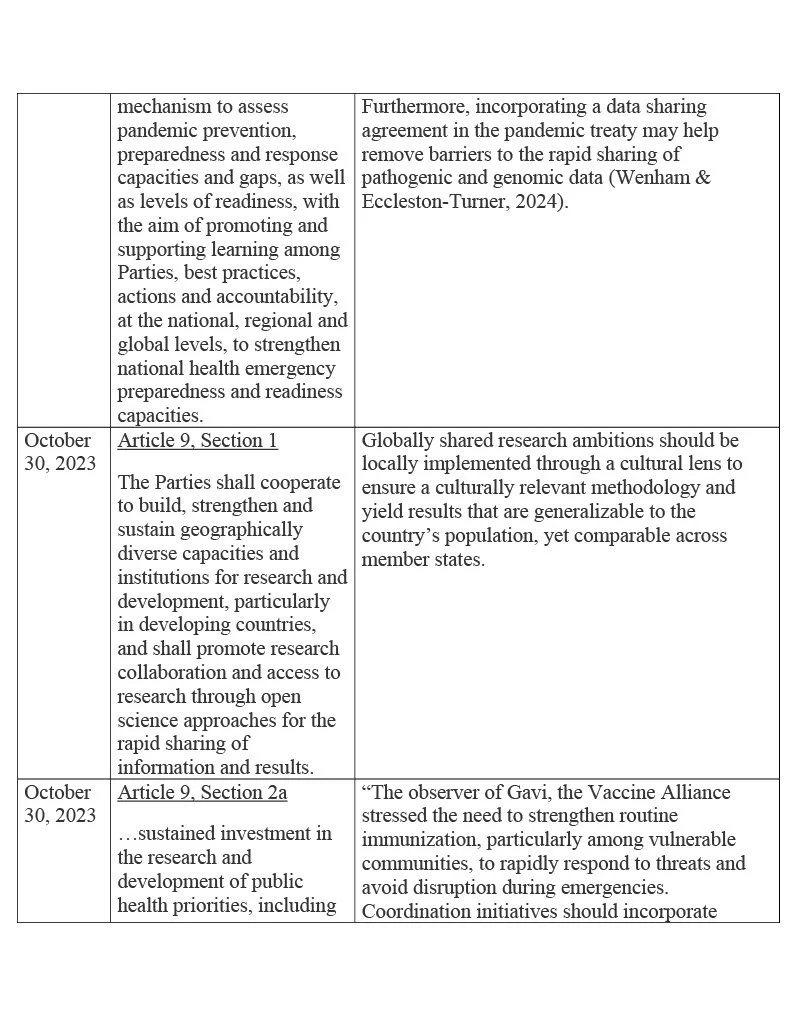
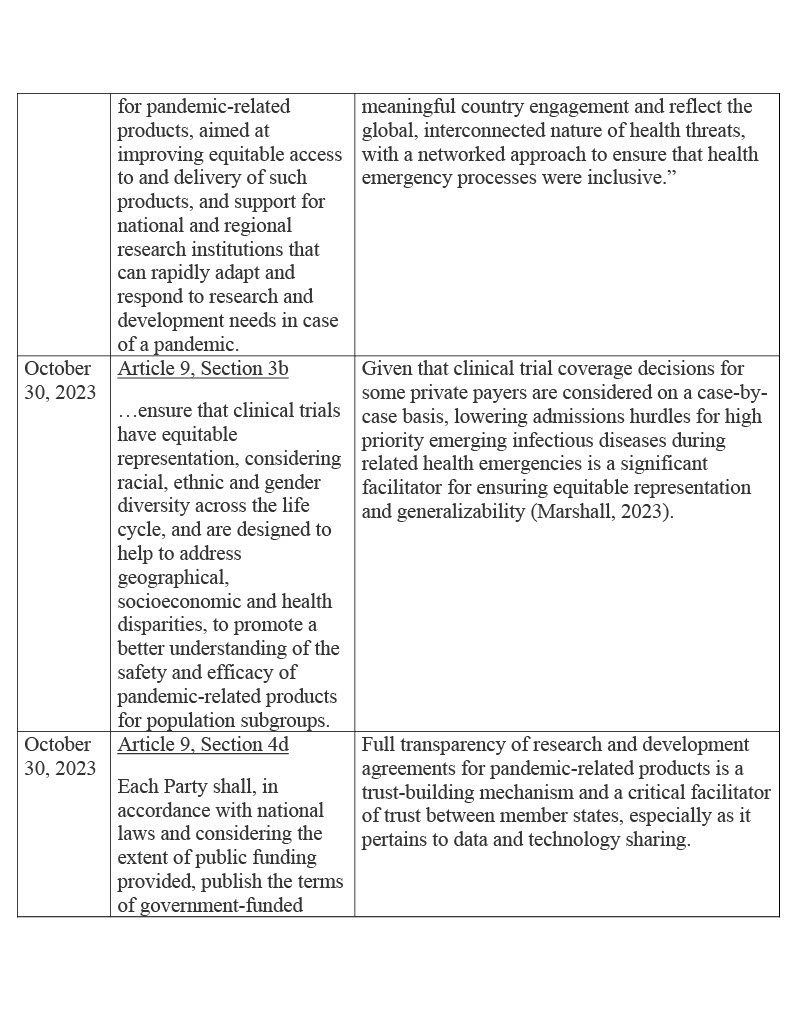
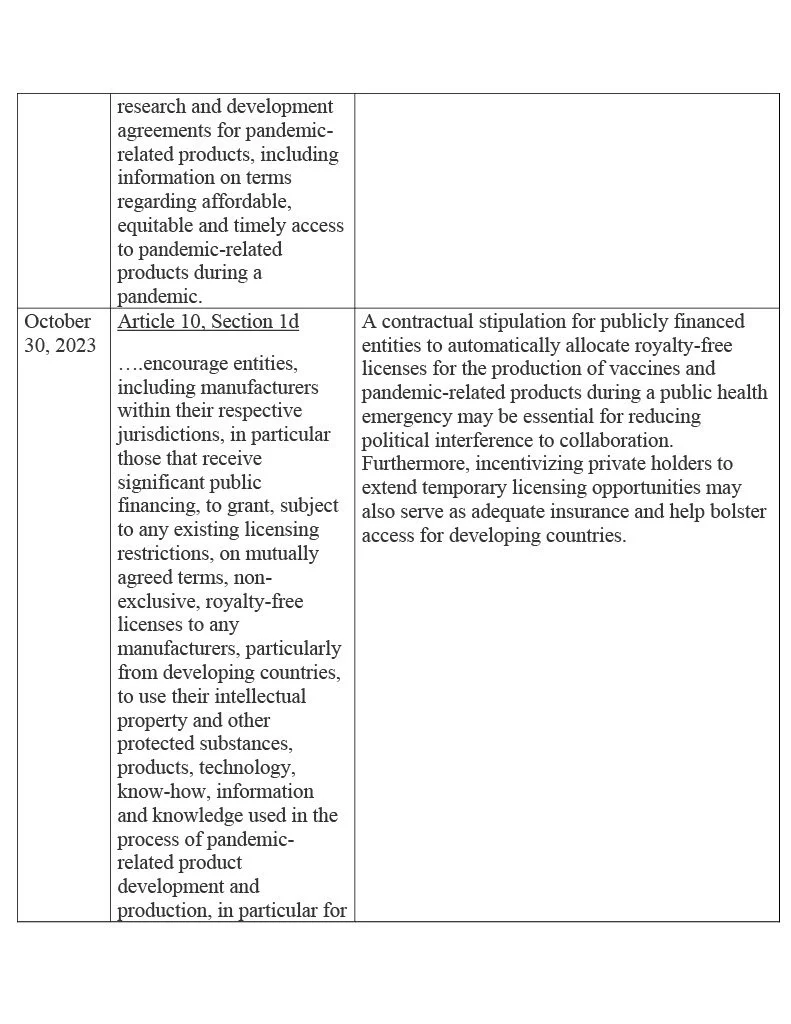
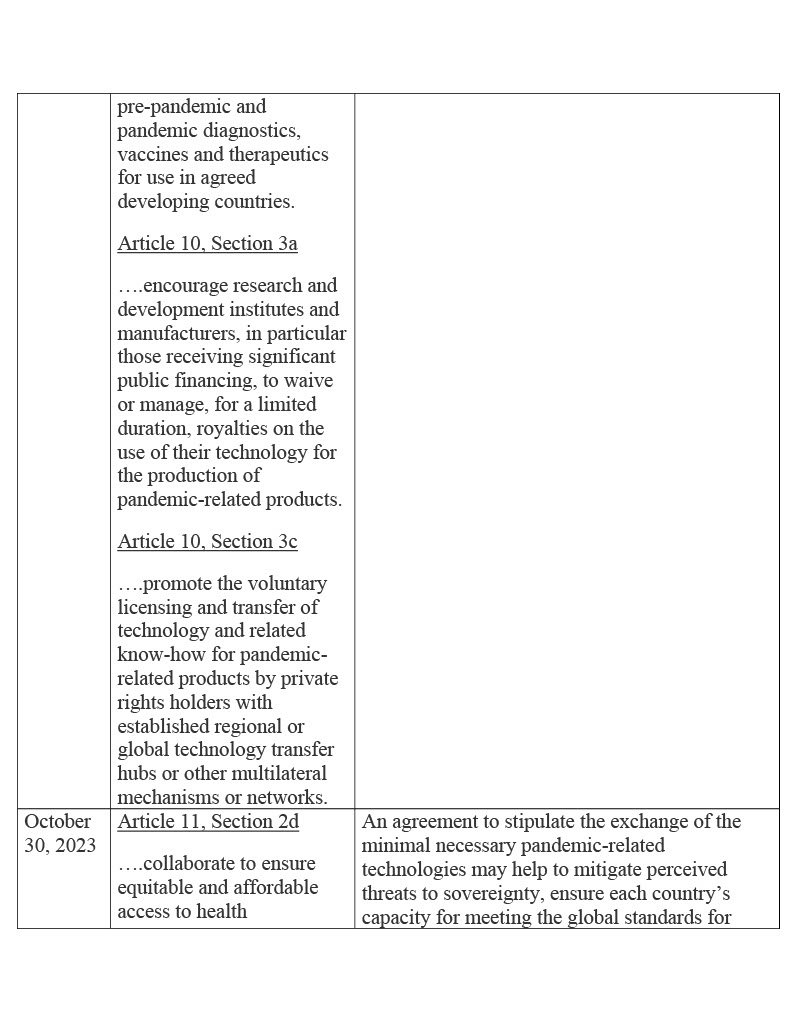
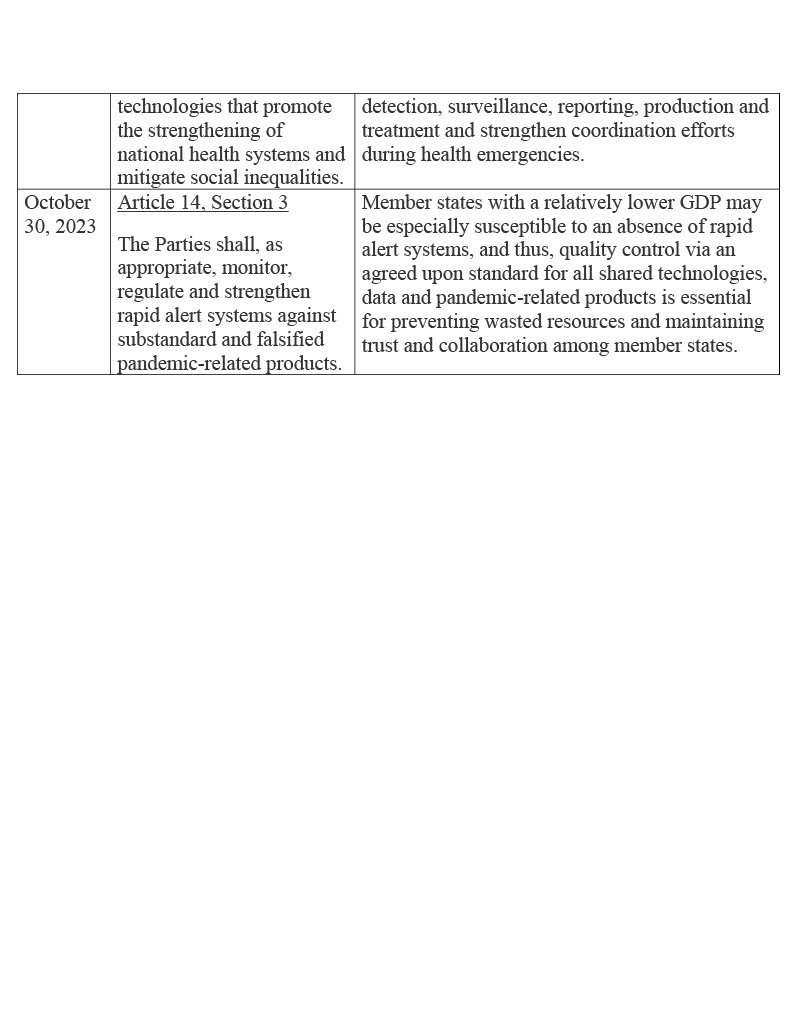
Table 1 below lists functional stipulations from different versions of the pandemic agreement negotiating text, along with viable operational definitions for added context:
Table 1: Operational Definitions for Equity based on the Terms of the Pandemic Agreement
Conclusion
One of the greatest benefits of competition between countries during the public health emergency is that competitiveness may have fueled technological and procedural innovation. The Global North’s development of new technology and the Global South’s advancement in infectious disease mitigation procedures supports the timing of such a collaborative agreement to help improve the world’s potential for a stronger coalition against future pandemics (Taylor, 2024). Despite concerns with national sovereignty, at the very least, exchanges of research methodologies and genetic information are imperative to effectively managing an emerging infectious disease with pandemic potential. That said, to ensure that concerns with sovereignty don’t interfere with guarantees of accountability to collaboration, and considering that both the Global North and South depend on collaboration to broaden access to vaccines, pathogenic data and high priority research, the most ethical route is perhaps to tie pandemic funding to global compliance standards by implementing a framework that requires contractual transparency, complementary exchanges of knowledge and technology, and reassurances of sovereignty during the centrally administrated mitigation of a global health emergency (Yu, 2024).
References
Azzariti, A. & Morich, D. (2023). Thematic Text Comparison: The Bureau’s text of the WHO CA+ for the consideration of the Intergovernmental Negotiating Body at its fifth (resumed session) and sixth meeting and the Negotiating Text of the WHO convention, agreement or other international instrument on pandemic prevention, preparedness and response (WHO Pandemic Agreement) for the consideration of the Intergovernmental Negotiating Body at its seventh meeting.
Marshall, J. (2023). Race-Based Disparities in Insurance Coverage Among Cancer Survivors. Diverse Perspectives on Wellness, 1(2), 1-10.
Ofongo, E.M., Raji, I. & Ofongo, T.M. (2024). Extrapolating Insights from the COVID-19 Pandemic for the Advancement of Global Health Policy and Practice: The Imperative of an International Pandemic Treaty. LAJOHIS, 6(1).
Proposal for negotiating text of the WHO Pandemic Agreement, 30 October 2023 for the consideration of the Intergovernmental Negotiating Body at its fourth meeting. World Health Organization, A/INB/7/3.
Schellekens, P. & Sourrouille, D.M. (2020). COVID-19 Mortality in Rich and Poor Countries: A Tale of Two Pandemics? World Bank Policy Research Working Paper, (9260).
Taylor, L. (2024). WHO pandemic treaty: “Torrent of fake news” has put negotiations at risk, says WHO chief. BMJ, 384(q243).
Wenham, C. & Eccleston-Turner, M. (2024). Will the pandemic treaty make it over the line? BMJ, 384(q395).
Yu, H. (2024). Proactively ensuring access to essential medical solutions: Lessons learned from the COVID-19 pandemic. In Intellectual Property Rights in Times of Crisis (pp. 83-103). Edward Elgar Publishing.
Zero draft of the WHO CA+, 1 February 2023 for the consideration of the Intergovernmental Negotiating Body at its fourth meeting. World Health Organization, A/INB/4/3.
Acknowledgements
This research was supported by Health Analytics & Visualizations.
Conflict of Interest
The authors declare no conflict of interest or financial incentive. The author’s relationships with the stakeholders and subject matter did not lead to unreasonable bias or compromise the objectivity of the research.
Rights and Permissions
Health Analytics & Visualizations supports the redistribution of its journal articles and content while also protecting its intellectual property from infringement. To request permission to republish our articles or content, email the Editor-in-Chief at info@stem4humanrights.com.
All Articles
Barriers and Facilitators to Racial Equity in K-12
Race-Based Disparities in Insurance Coverage Among Cancer Survivors
Social Dynamic Response Theory
The Global Impact of the COVID-19 Pandemic on Maternal Mortality
Reducing the Body Count During the Next Pandemic
Math Anxiety Interventions to Address the STEM Gender Gap for Girls
Changes in Sea Surface Temperature and Cyclone Intensity over the Past Two Centuries