
The Global Impact of the COVID-19 Pandemic on Maternal Mortality
Marshall, J.
Author correspondence: info@stem4humanrights.com
Cite this article: Marshall, J. (2023). The Global Impact of the COVID-19 Pandemic. Diverse Perspectives on Wellness, 1(4), 1-9.
Abstract
During the first full year of the COVID-19 pandemic, maternal and infant mortality rates increased for many countries while remaining steady and even declining in others, leading to questions regarding the common denominators that may have influenced access to maternal health care and safety. In addition to the three delays (i.e., a delay in seeking health care after the sudden onset of labor, a delay in reaching a health facility, and a delay in being assisted once the health facility is reached), Pearson’s correlation analysis of maternal health data from 20 countries revealed a significant negative relationship between midwives per 1,000 live births and maternal and infant mortality rates. Results suggest the critical importance of midwives, perhaps especially during pandemics and wartime when higher stress levels can compromise the health and safety of both new and expectant mothers and infants.
Keywords: maternal mortality, infant mortality, midwives, COVID-19, global health
Introduction
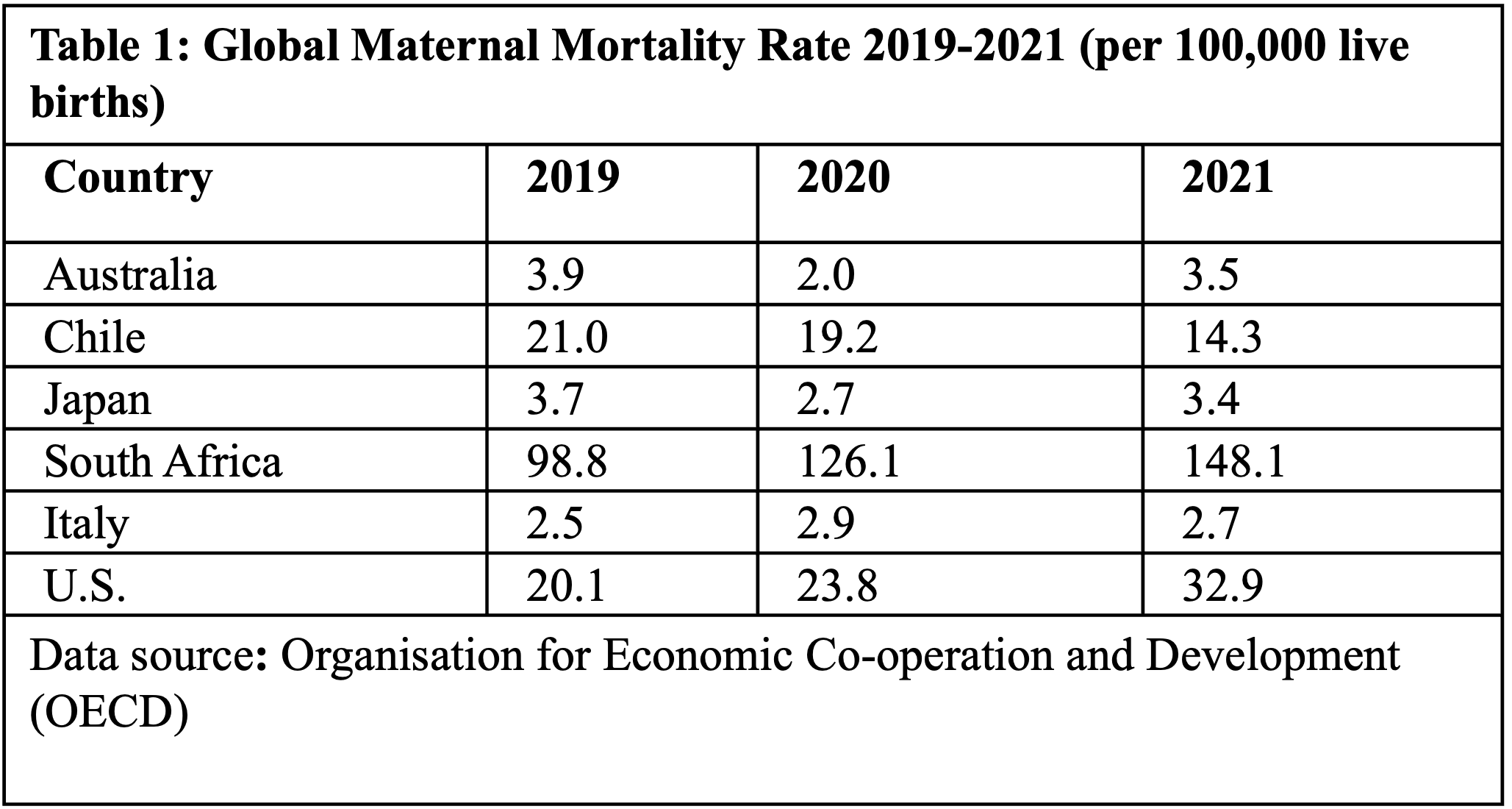
With few exceptions around the world, many countries experienced a sudden fluctuation in maternal mortality rates during the first few years of the COVID-19 pandemic (Alabi et al., 2022). After the start of the pandemic, maternal mortality rates increased dramatically for both the U.S. (20.1 in 2019; 23.8 in 2020; 32.9 in 2021) and South Africa (98.8 in 2019; 126.1 in 2020; 148.1 in 2021). Chile, on the other hand, experienced steady decreases (21.0 in 2019; 19.2 in 2020; 14.3 in 2021); while perennially low rates in Australia (3.9 in 2019; 2.0 in 2020; 3.5 in 2021), Italy (2.5 in 2019; 2.9 in 2020; 2.7 in 2021), and Japan (3.7 in 2019; 2.7 in 2020; 3.4 in 2021) remained fairly consistent (see Table 1).
Research supports most maternal deaths as attributable to one of the following three delays: 1) A delay in seeking health care after the sudden onset of labor, 2) a delay in reaching a health facility, and 3) a delay in being assisted once the health facility is reached (Onambele et al., 2022). While delays in accessing maternal health care are a perennial issue in some countries, these delays can be even further impacted by overlapping crises as was the case for Afghanistan where a mid-pandemic political turnover in 2021 led to withdrawn health care funding which compounded the negative impact on what was already one of the world’s lowest maternal mortality rates at 620 deaths per 100,000 live births (Tharwani et al., 2022). In fact, 75% of the countries who registered a high maternal mortality rate in 2008 were at war, and while the morality of diverting health care funding during overlapping crises remains an interesting philosophical argument, there’s little argument that pandemics, much like wartime, create competition that can strain the distribution of resources, services, supplies, and personnel (Onambele et al., 2022). The isolated impacts of COVID-19 on each country’s maternal mortality rate are likely a reflection of the impact of COVID lockdown measures on the three delays that become more prevalent during crises, the ability of health care institutions and patients to prevent and circumvent the “three delays”, overall effectiveness in preventing COVID transmission, population density, and geographic size. Although many countries and their citizens experienced region-specific barriers to accessing maternal health care during COVID-19 pandemic that may only be applicable to the given population, examining their unique approaches responses to maternal health care challenges during times of disaster and institutional strain offers an opportunity for both retrospection and improved emergency preparedness as it pertains to mitigating loss of life for new and expectant mothers and infants and loss of resources.
Clinical Characteristics of COVID in Maternal Health Cases
Non-obstetric causes of maternal mortality (i.e., causes not directly related to pregnancy and childbirth) commonly include severe hemorrhage, infection, high blood pressure and unsafe abortion, and account for a majority of all maternal deaths but become an even bigger issue in the context of pandemics and within endemic regions (WHO, 2023). On the African continent, malaria is the number one non-obstetric cause of maternal mortality, and the prevalence of plasmodium falciparum, the deadliest parasitic causative agent of malaria in Africa, is seasonally high in young women (e.g., in Mali, 42.2% in the rainy season vs. 11.5% in the dry season) (Onambele et al., 2022). Globally, COVID-19 is an especially difficult non-obstetric complication. A Latin American study showed that for women who experienced COVID-associated maternal death, 60.3% of COVID cases were detected in the third trimester and 76.9% experienced preterm delivery (Maza-Arnedo, 2022). Unvaccinated pregnant women may especially struggle with receiving an accurate prognosis, succumb to a less predictable course of COVID disease, and face an increased likelihood of pre-term births and other pregnancy complications (Atak, 2022). Among unvaccinated mothers in Turkey, the COVID-associated maternal mortality rate (156.3 deaths per 100,000) was 19.9% higher than the overall maternal mortality rate (128.0 deaths per 100,000), suggesting COVID testing prior to the third trimester and maternal health vaccinations as a means by which to reduce maternal mortality (Atak, 2022).
Concerns of Maternal Healthcare Patients
Given the political upheaval in Afghanistan during COVID and its impacts on gender equality, especially as it pertains to access to health care and health care employment, it may come as no surprise that 40% of Afghan women identified safety as a primary concern when seeking medical assistance. However, while accessible maternal health care in Afghanistan is a perennial issue, during COVID, the concern for personal safety while seeking health care became a shared phenomenon among women across the globe, even among those in countries with low maternal mortality rates (Tharwani et al., 2022). One Italian study acknowledges the increased prevalence of negative emotional experiences during the pandemic as a potential driver of low quality pregnancy experiences and poor maternal health outcomes. Basic emotions related to childbirth expectations among a pre-pandemic and a mid-pandemic cohort of mothers were significantly different based on chi-square tests that evaluated joy (pre-pandemic, 63%; mid-pandemic, 17%, p < 0.00001), anticipation (26.5%; 14.0%, p < 0.01), surprise (10.5%; 2.5%, p < 0.01), trust (7.0%; 0.5%, p < 0.001), fear (7.5%; 49.0%, p < 0.0001), and sadness (0.5%; 10.5%, p < 0.0001). In both cohorts, differences in negative physical sensations (16.5%; 13.5%, p < 0.7) and positive physical sensations (3.5%; 1.0%, p < 2.8) were not significantly different; however, more positive psychological constructs of awareness (7.0%; 0.5%, p < 0.001), closeness (49.5%; 0.5%, p < 0.0001), empathy (5.5%; 1.0%, p < 0.05), love (13.0%; 3.0%, p < 0.001), safety (38.0%; 7.5%, p < 0.0001) and serenity (25.5%; 1.0, p < 0.0001) were overwhelmingly present in the pre-pandemic cohort, whereas negative psychological constructs of anxiety (3.0%; 32.5%, p < 0.0001), danger (0%; 26.0%, p < 0.00001), loneliness (1.0%; 53.5%, p < 0.0001), restriction (19.0%; 41.99%, (p < 0.00001), self-doubt (1.0% vs 9.0%, p < 0.001), and worry (1.0% vs 19.5%, p < 0.0001) were more prevalent in the mid-pandemic cohort of mothers (Rusconi et al., 2023).
Skilled & Unskilled Labor
In Japan, through sponsorship by a program called Konnichiwa Akachan Jigyo, local municipalities conduct home visits to new mothers within 4 months after delivery to help expand post-natal care beyond hospital discharge. However, during the pandemic, the skilled health care workers who support this program cited difficulty in talking face-to-face, providing support for partners of maternal health patients, offering assistance to families, and dealing with their own anxiety in regard to being a potential source of infection (Furudate, 2023). The intensity of COVID lockdowns has meant delays in access to maternal health care that in some countries, led to an increase in deliveries and post-natal care assisted by unskilled people. Studies have linked hemorrhage, one of the leading causes of maternal death, to deliveries assisted by unskilled people, performed at home or in ill-equipped primary health care centers without access to consumables or transfusion (Onambele et al., 2022). In India, 89% of childbirths in 2020 were skilled birth assisted deliveries, and their maternal mortality rate of 97 deaths per 100,000 is well below WHO’s sustainable development goal of 140 deaths per 100,000. In Senegal, their 75% attendance rate for skilled healthcare workers during live births is perhaps reflected in their maternal mortality rate of 261 deaths per 100,000, and Afghanistan’s maternal mortality rate of 620 deaths per 100,000 is at least partially attributable to the fact that only 62% of births were attended by a skilled health care worker (Tharwani et al., 2022; UNICEF, 2020). This perceived tendency for countries with a lower percentage of births attended by a skilled health care worker to have a higher maternal mortality rate led to our research question, “During the first full year of the global COVID-19 pandemic, was there a significant relationship between rates of ob-gyns and midwives per country and lower rates of maternal and infant mortality?”
Methods
Disease surveillance requires the data collection infrastructure necessary to find new cases and maintain accurate records of pre-existing disease. However, pandemic and wartime conditions may create difficulties with estimation of maternal mortality given the increased potential for deliveries performed outside of healthcare facilities, attended by unskilled people, and deceased new and expectant mothers with undocumented pregnancies (Onambele et al., 2022). The nature of estimate generation during crises means that shifting conditions within the sample population may lead to a larger sampling error where certain sub-populations may not be well-represented. Regardless, measures of certainty (or uncertainly) are usually reflected in the standard error, coefficient of variation (i.e., variability), and confidence interval and offer reassurance regarding how much of an emphasis to place on pandemic-era estimates. Maternal mortality is defined as the death of a woman either while pregnant or within 42 days after the pregnancy’s termination from any cause related to pregnancy, its management, and/or complications from pregnancy or childbirth, with the exception of unintentional or incidental cases (Tharwani et al., 2022). According to WHO guidelines, methods to count stillbirths across countries vary, and thus, when comparing maternal mortality rates globally, excluding stillbirths from counts is considered a best practice in order to ensure reliable data. There is much overlap in global methods to track maternal mortality rates (e.g., demographic surveillance, maternal death surveillance and response systems, health record review studies, prospective cohort studies, confidential inquiries into maternal deaths, reproductive-age mortality surveys, direct or indirect sisterhood methods and mathematical modeling); however, maternal mortality and infant mortality rates utilized for these analyses are primarily modeled estimates from OCED (Organization Economic Co-operation and Development), with national estimates from UNICEF (United Nations International Children's Emergency Fund) utilized where modeled estimates were not available (Onambele et al., 2022). This study proceeded with a correlation analysis to determine if rates of ob-gyns and midwives per country were associated with lower rates of maternal and infant mortality.Pearson's r formula (r=∑(xi−x̄)(yi− ȳ)√ (∑(xi−x̄)2(yi−ȳ)2) ½) for measuring correlation remains remarkably unchanged for a 100-year old index and is the most popular statistical measure of association between variables (Lee Rodgers & Nicewander, 1988). R 4.2.0 was used to analyze these data, and results were interpreted based on a significance level of p <.05. Countries included in the analysis were those with searchable estimates for either maternal or infant mortality rate and either ob-gyns or midwives per 1,000 live births (see Table 2).
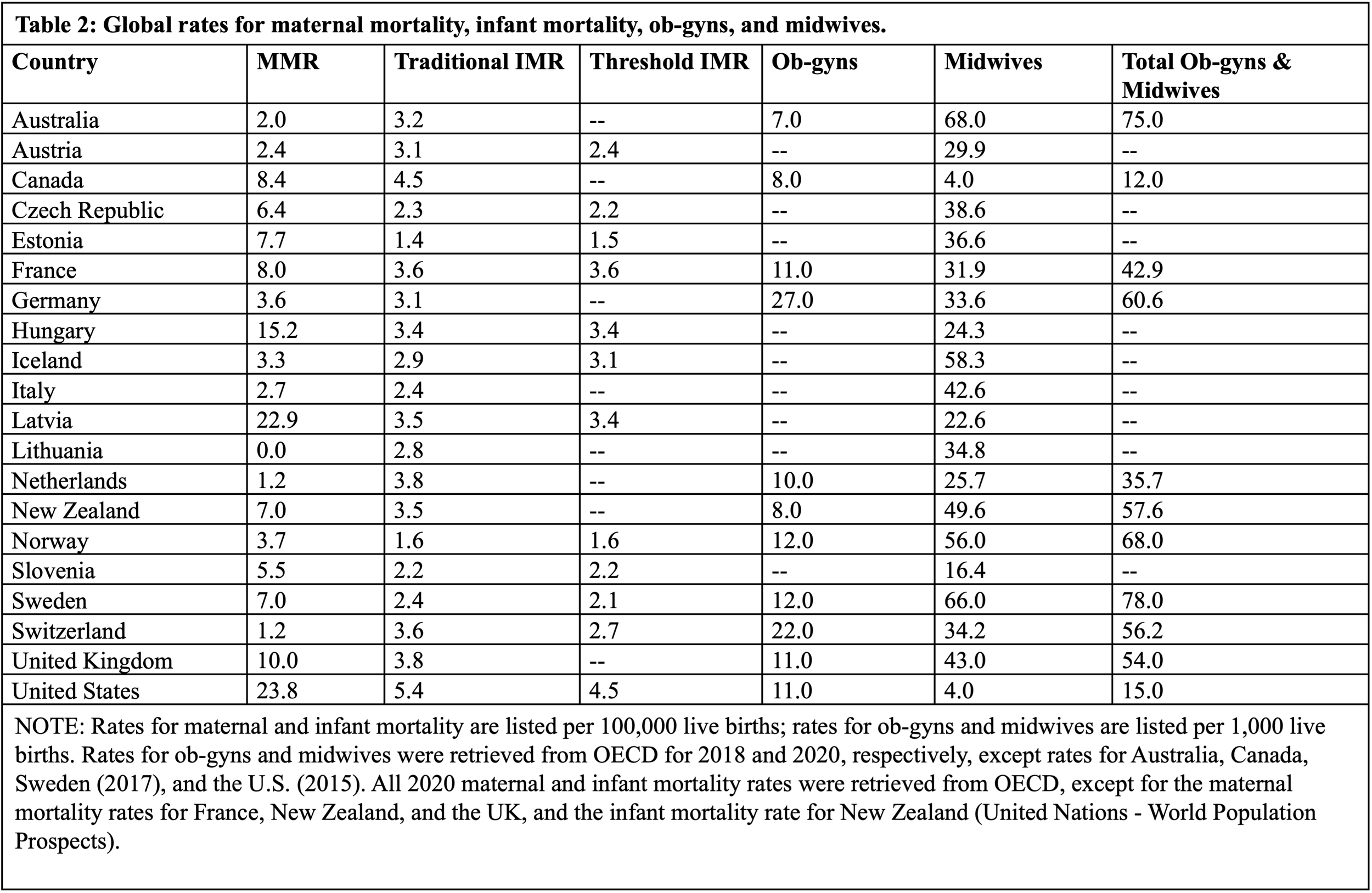
Traditional infant mortality rates with no minimum threshold of gestation period or birthweight and threshold infant mortality rates (also referred to as corrected mortality rates) whose criteria require a minimum gestational age of 22 weeks or 500 grams for a child to be considered a live birth were analyzed against rates of ob-gyns and midwives as available. A limitation of this analytic approach is that a number of countries tend to report combined rates for nurses and midwives per 1,000 people rather than rates for midwives alone per 1,000 live births or ob-gyns alone per 1,000 live births, and thus, those countries were not able to be included in this analysis. Italy, for example, provides rates for midwives alone and nurses and midwives in combination (6.3 nurses and midwives per 1,000 people vs 42.58 midwives per 1,000 live births), but given the vast differences in calculating the numerators and denominators for each individual rate, inclusion of those countries with only a combined rate of nurses and midwives per 1,000 people was not feasible for this analysis. Lastly, it must be noted that as far as the variables for midwives and total ob-gyns and midwives are concerned, the definition of midwife varies from country-to-country. OECD data represents practicing midwives, Canada’s rate reflects those midwives who are professionally active, and the U.S. rate reflects midwives who are licensed to practice.
Results
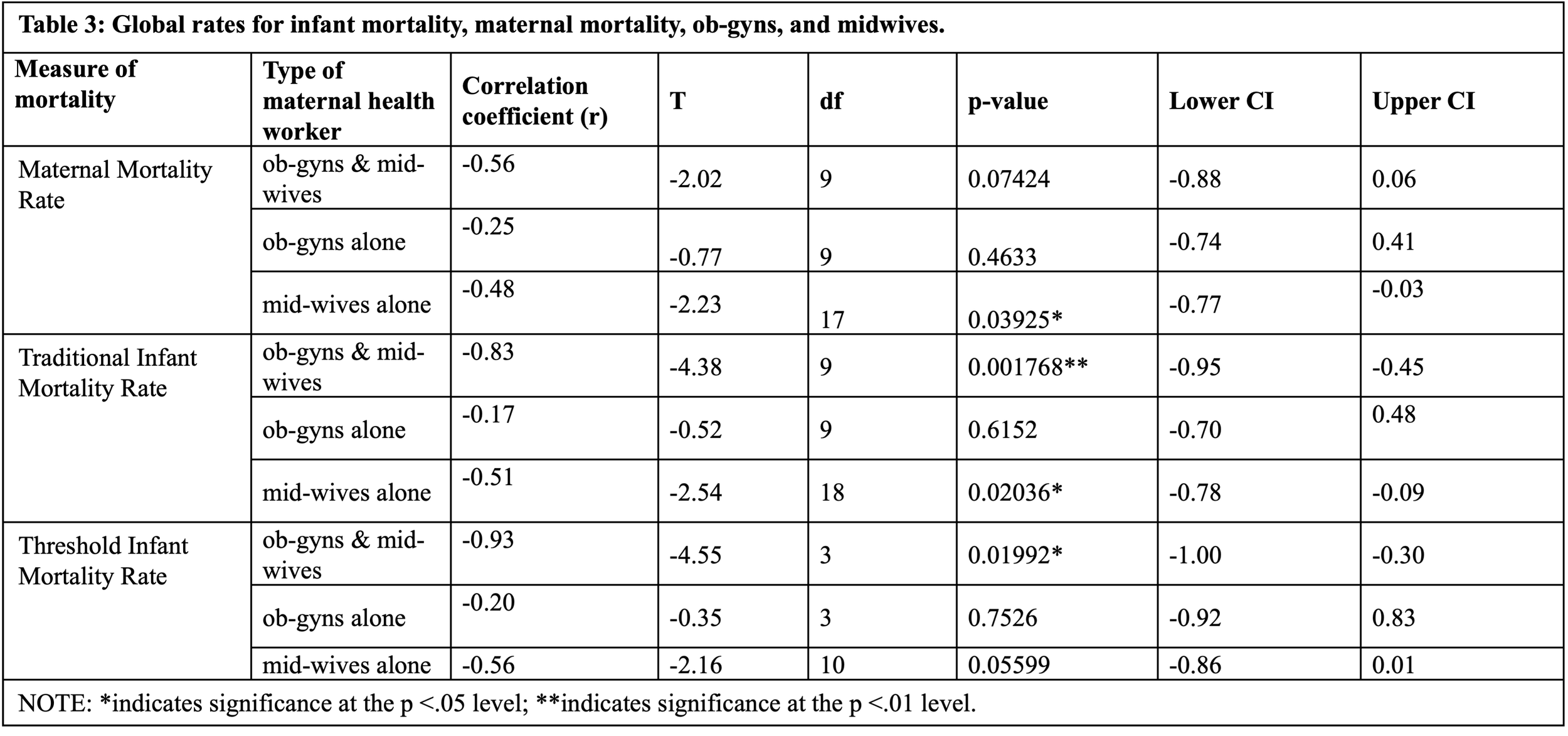
This study performed several tests for correlation between each country’s rate of skilled maternal health workers and maternal health outcomes based on the available data shown in Table 2. Among findings significant at the p < .05 level were strong negative correlations between the total rate of ob-gyns and midwives per 1,000 live births and both the traditional infant mortality rate (r = -0.83, p = .002, 95% CI: -0.95, -0.45) and the threshold infant mortality rate (r = -0.93, p = .02, 95% CI: -1.0, -0.3). Moderately negative correlations were revealed between midwives alone per 1,000 live births and both maternal mortality rate (r = -0.48, p = .04, 95% CI: -0.77, -0.3) and traditional infant mortality rate (r = -0.51, p = .02, 95% CI: -0.78, -0.09). Additional results from these analyses are available in Table 3.
Discussion
Results reveal that both midwives alone and combinations of ob-gyns and midwives are critical supports for maternal and infant health care; however, no significant correlations were revealed for ob-gyns and either maternal or infant mortality rates. Still, more research is needed to determine the impact of factors beyond maternal healthcare workers on maternal and infant health, especially during times of crisis. For example, while the safety of home births is the subject of much debate, there is an important distinction between contemporary planned home births that intentionally take place at home and those home births attended by unskilled workers and in less-than-ideal conditions (Pintassilgo, 2023). In Portugal, between 1995 and 2020, home births performed by skilled health care workers were positively correlated with reduced maternal mortality whereas those attended by unskilled workers were correlated with higher rates of maternal mortality. At the start of the pandemic, however, while the rate of home births in Portugal increased by at least 33% compared to the previous year and 93.3% of these home births were attended by a doctor, midwife, or nurse (suggesting a high rate of skilled birth attendance during both home and hospital births), the maternal mortality rate still increased from 10.4 to 20.1 deaths per 100,000 in 2020. But in 2021, Portugal’s maternal mortality rate dropped to 8.8 deaths per 100,000. Whether this is attributable to a population-level adjustment over time to mitigate the three delays, the lifting of pandemic-era restrictions in 2021, or a shift in maternity health COVID testing protocols is up for debate and highlights the need for additional analyses to help quantify various systemic and social impacts on health care during crises (Pintassilgo, 2023). This narrative also reveals the complexity behind reassuring safety and stability in maternal health care during the pandemic, and multiple studies suggest paying more attention to patient concerns, evaluating pre- and mid-crisis emotional constructs, and disaggregating health and emotional experiences for new and expectant mothers during crises as critical strategies to help mitigate stress and aide early detection of increasing mortality rates. In the U.S., although an overall 18.4% increase in the maternal mortality rate during the first full year of the pandemic was not especially pronounced, a 44.44% increase among Hispanic Americans and a 25.68% increase among Black Americans suggests that early responses to populations with notable increases in morbidity may help curtail issues with delays, jumpstart mitigation efforts and further reduce negative impacts. Also, scaling up the maternal health workforce is a practical means towards increasing maternal health visits, and Ethiopia provides another interesting case study to help support this narrative. In 2005, the percentage of pregnant women in Ethiopia who received any antenatal care from a skilled provider was 28%. In 2009, the Ministry of Health of Ethiopia launched a master’s degree program to significantly increase capacity for emergency obstetric care services including surgery. By 2016, the percentage of women in Ethiopia who received any antenatal care increased by 82%, the percentage of women who received 4 or more antenatal care visits increased by 68%, and the percentage of women who received antenatal care during their first trimester increased by 81% (Ayele et al., 2021). Although Ethiopia’s efforts to rapidly scale their maternal health workforce took place prior to the COVID-19 pandemic, a brief history of this initiative to increase support for the maternal healthcare workforce helps clarify a feasible pathway towards improving maternal health outcomes, especially in countries with high maternal mortality.
Limitations
Several countries were unable to be included in the analysis due to a preference for exclusively reporting combined counts for nurses and midwives, and it’s likely that a low density of midwives and ob-gyns may help explain this reporting preference. Moreover, estimates for ob-gyns alone per 1,000 live births were difficult to retrieve, and thus, a potential limitation of this analysis is that more complete data for ob-gyns may help to improve the global perspective regarding their importance to maternal health outcomes. Although this study did not specifically address social influences as a predictor of maternal and infant mortality, one study revealed Chile’s dramatic increase in women’s educational levels from 3.5 in 1957 to 12.0 in 2007 as the strongest influence on a steadily declining maternal mortality rate, which is especially notable given Chile’s 1989 abortion ban (Koch et al., 2012). However, despite the influence of women’s education levels on the uptake of maternal health care services, avoidable maternal and infant mortality deaths have been at least qualitatively associated with healthcare funding lower than 6% of a country’s GDP, inequalities in freedom of choice, and lack of autonomy in care, and further research should continue to investigate specific gender inequality-related impacts as predictors of maternal and infant health outcomes (Onambele et al., 2022; Weiland et al., 2021).
Furthermore, while admissions decisions can be complicated and influenced based on available beds and appropriate skill available on site, more research is needed to assess and bolster the capacity of ICUs to handle severe maternal health cases. Despite 90.4% of Latin American COVID-associated maternal death cases displaying organ dysfunction during their first consultation, only 64.8% of women were admitted to critical care (Maza-Arnedo, 2022). Lastly, it must be noted that perspectives on primary causes of maternal death during COVID often differ between patients and providers. South African patients attribute avoidable maternal deaths to delays in accessing medical help (29.0%), not having received antenatal care (16%), lack of information (10.2%) and declined medication/surgery/advice (6.6%). Meanwhile, South African administrators attribute maternal deaths to not having the appropriate skill available on site (9.8%), lack of healthcare facilities (ICU) (9.7%), lack of information (9.0%), and delays in attending to patients due to overburdened service (7.1%) (World Health Organization – African Region, 2023). That said, this study wishes to align with a well-supported idea in research that each pregnancy and maternal death is unique, and “considering maternal mortality as a potentially avoidable phenomenon, each maternal death would deserve a qualitative analysis at its base (Pintassilgo, 2023).”
References
Atak, Z., Rahimli Ocakoglu, S., Topal, S. & Macunluoglu, A.C. (2022). Increased maternal mortality in unvaccinated SARS-CoV-2 infected pregnant patients. Journal Of Obstetrics and Gynaecology, 42(7), 2709-2714.
Ayele, A.A., Tefera, Y.G. & East, L. (2021). Ethiopia’s commitment towards achieving sustainable development goal on reduction of maternal mortality: There is a long way to go. Women's Health, 17, 17455065211067073.
Donati, S., Buoncristiano, M., Lega, I., D’Aloja, P. & Maraschini, A. (2021). The Italian obstetric surveillance system: Implementation of a bundle of population-based initiatives to reduce haemorrhagic maternal deaths. PLoS One, 16(4), e0250373.
Furudate, A., Takahashi, K. & Kinjo, K. (2023). Difficulties experienced by health care professionals who performed home visits to screen for postpartum depression during the COVID-19 pandemic: A qualitative study in Japan. BMC Health Services Research, 23(1), 1-9.
Koch, E. (2013). Impact of reproductive laws on maternal mortality: The Chilean natural experiment. The Linacre Quarterly, 80(2), 151-160.
Lee Rodgers, J. & Nicewander, W.A. (1988). Thirteen ways to look at the correlation coefficient. The American Statistician, 42(1), 59-66.
Maza-Arnedo, F., Paternina-Caicedo, A., Sosa, C.G., de Mucio, B., Rojas-Suarez, J., Say, L. ... & Colomar, M. (2022). Maternal mortality linked to COVID-19 in Latin America: Results from a multi-country collaborative database of 447 deaths. The Lancet Regional Health–Americas, 12.
Mendez-Dominguez, N., Santos-Zaldívar, K., Gomez-Carro, S., Datta-Banik, S. & Carrillo, G. (2021). Maternal mortality during the COVID-19 pandemic in Mexico: A preliminary analysis during the first year. BMC Public Health, 21(1), 1-9.
National Department of Health – (includes data for second year of the COVID-19 pandemic). Annual Report for 2021. Retrieved 1 December, 2023, from https://www.health.gov.za/wp-content/uploads/2023/09/Saving-Mothers-Report-2021.pdf
Pintassilgo, S., Santos, M.J., Trindade, I. & Neves, D.M. (2023). Home birth in Portugal—A comprehensive analysis based on official statistical data. Social Sciences, 12(6), 314.
Tharwani, Z.H., Kumar, P., Shaeen, S.K., Islam, Z., Essar, M.Y. & Ahmad, S. (2022). Maternal mortality in Afghanistan: Challenges, efforts, and recommendations. Clinical Epidemiology and Global Health, 15, 101038.
Tikkanen, R., Gunja, M.Z., FitzGerald, M. & Zephyrin, L. (2020). Maternal mortality and maternity care in the United States compared to 10 other developed countries. The Commonwealth Fund, 10, 22.
UNICEF, State of the World's Children, Childinfo, and Demographic and Health Surveys. Retrieved 1 December, 2023, from https://data.unicef.org/resources/resource-type/datasets
World Health Organization – African Region. Analytical Fact Sheet. March 2023. Retrieved 1 December, 2023, from https://files.aho.afro.who.int/afahobckpcontainer/production/files/iAHO_Maternal_Mortality_Regional_Factsheet.pdf
World Health Organization – Preterm birth. Key Facts, May 2023. Retrieved 1 December, 2023, from https://www.who.int/news-room/fact-sheets/detail/preterm-birth
Yu, D., Zhang, L., Yang, S., Chen, Q. & Li, Z. (2021). Trends, causes and solutions of maternal mortality in Jinan, China: The epidemiology of the MMR in 1991–2020. BMC Public Health, 21, 1-11.
Acknowledgements
This research was supported by Health Analytics & Visualizations.
Conflict of Interest
The authors declare no conflict of interest or financial incentive. The author’s relationships with the stakeholders and subject matter did not lead to unreasonable bias or compromise the objectivity of the research.
Rights and Permissions
Health Analytics & Visualizations supports the redistribution of its journal articles and content while also protecting its intellectual property from infringement. To request permission to republish our articles or content, email the Editor-in-Chief at info@stem4humanrights.com.
All Articles
Barriers and Facilitators to Racial Equity in K-12
Race-Based Disparities in Insurance Coverage Among Cancer Survivors
Social Dynamic Response Theory
The Global Impact of the COVID-19 Pandemic on Maternal Mortality
Reducing the Body Count During the Next Pandemic
Math Anxiety Interventions to Address the STEM Gender Gap for Girls
Changes in Sea Surface Temperature and Cyclone Intensity over the Past Two Centuries